NoCal Kaiser HMO SBC
NoCal Kaiser DHMO_SBC
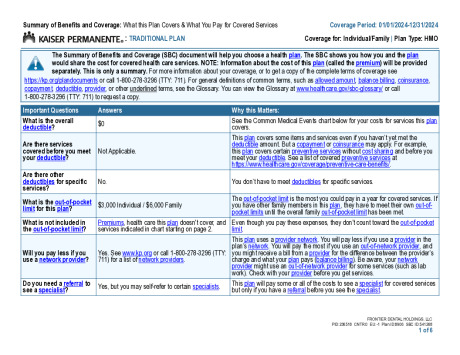
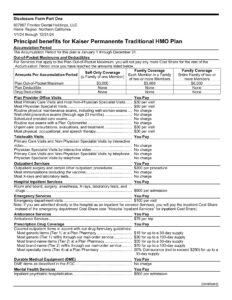
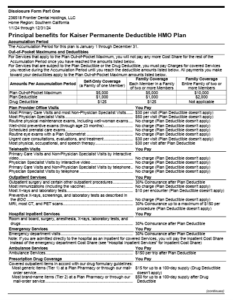
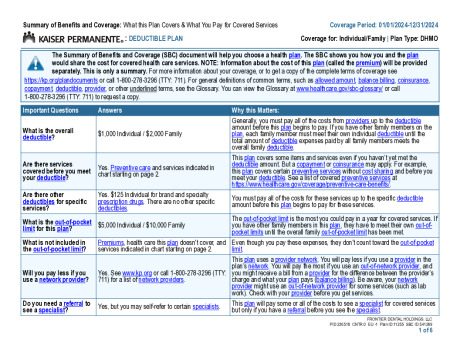
Kaiser SoCal HMO SBC
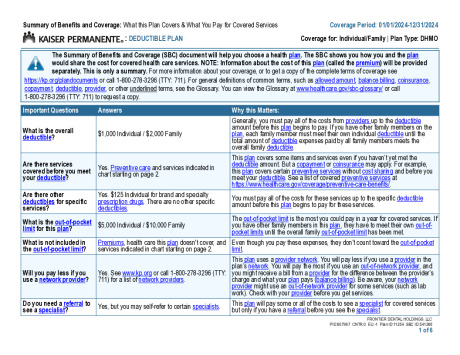
Kaiser SoCal DHMO SBC
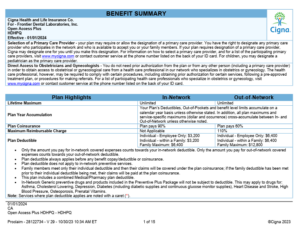
Denbright - 2025 Cigna Medical HDHPQ SBC
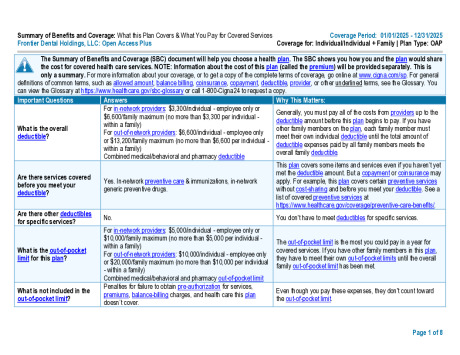
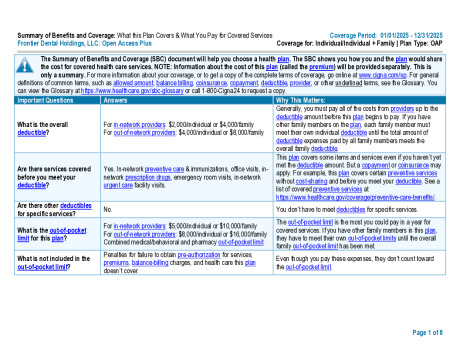
Denbright - 2025 Cigna OAP 2K SBC
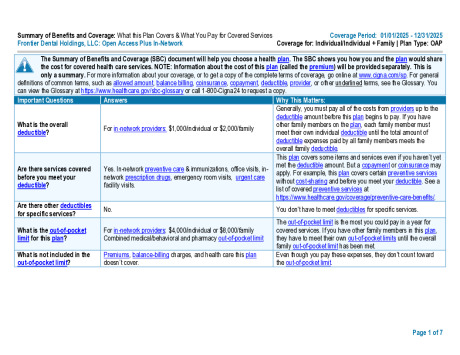
Denbright - 2025 Cigna OAP 1K SBC
2024 Cigna Medical HDHPQ SPD
2024 Cigna Medical OAP 2K SPD
2024 Cigna Medical OAP 1K SPD

Cigna Know Your Lemons
Preparing for Annual Physical









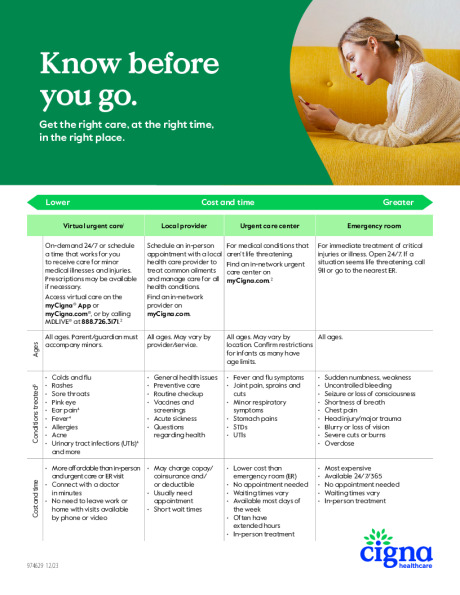
Know before you go